Habits

Rituals, obsessions, checking, hoarding, compulsions, impulse control, self-awareness reduced with neurofeedback.
Thoughts

Intrusive, obstructive, self-deprecating negative thoughts, internal dialogue, voices, delusions and hallucinations.
Positive Outlook

Mood control, social awareness, focus, optimism, motivation, outlook and goal-directed behaviour restored.
Personalised Brain Training improves OCD Symptoms.
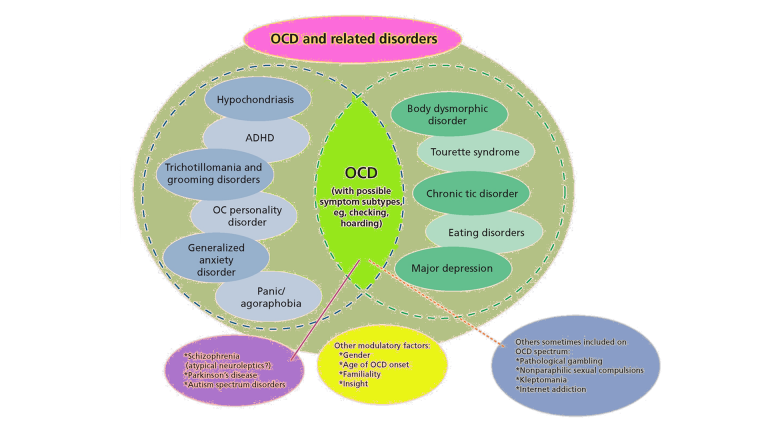
Obsessive-Compulsive Disorder (OCD) is defined as presence of obsessions, such as intrusive thoughts that are internally combatted or assuaged with ritual behavour; and/or compulsions, such as repetitive or checking behaviour, aimed at reducing anxiety and distress. It is often comorbid with other mood disorders, anxieties and trauma manifestations; and symptoms can be similar to both autism and schizophrenia.
Manifestations are time-consuming and lead to various lost social opportunities; whether missing out on interaction, not portraying one’s confident best, desynchronising and not living in the moment, the competition between internal thought processes and living in our environment is imbalanced. We aim to restore a healthy sense of self, reduce anxieties, create a healthy sense of detachment, improve sleep, focus, productivity and mood control. These attributes all have neural correlates, as in, brain areas or networks, with a measurable EEG signal that we can analyse into band components. There are various relationships between these that can be assessed and trained with neurofeedback, to improve cortical functioning.
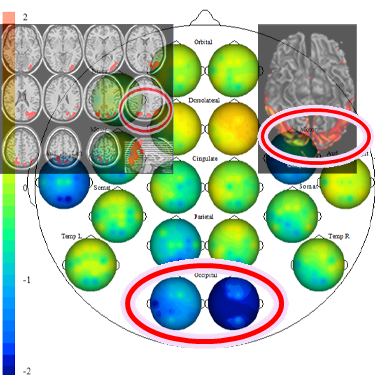
With a brain map and neurofeedback, we look to attribute character traits and behaviour patterns to the function of specific brain areas and general networks. This is a scientific, evidence-based approach, and it is real: A brain map shows us whether individual, functional brain areas are effectively repurposing limbic drives into pro-social behaviour, with regard to their specific function.
We can measure brain rhythms real-time, and give the brain feedback as to whether it is achieving efficient patterns – while watching a movie of choice, the volume or picture size changes slightly and temporarily when underperforming, and the brain – subconsciously – adapts its behaviour, and we see a learning curve. All the while, the individual is consciously absorbed in the movie, their preconscious mind does the work and training can be considered passive, and enjoyable.
OCD symptoms vary, and there are usually many comorbid challenges, such as various anxieties; mood control, sleep and focus issues; and deficits in social interaction.
With a brain map, we take a personalised approach. Identifying which brain areas and networks are dysrythmic allows us to structure an individualised training plan, independent of diagnosis, which we do not provide. The process is holistic, as we find that it takes the combined effect of multiple functional brain areas to improve productivity, motivation and social integration, something we can mostly achieve over 10-20 three hour sessions (individual brain maps and cases differ). We offer these as weekly sessions or intensive courses with two sessions per day over a week.
We are showing the brain what it feels like to perform in a more efficient manner. In this sense, the process is organic. It is evidence-based and non-invasive.
Scope of Neurofeedback Training for OCD
Behaviour patterns we can seek to address with neurofeedback training include the following:
– excessive worries, intrusive thoughts and ruminations
– guilty ruminations and negative outlook
– repetitive restrictive behaviour
– letting go – emotional and physical hoarding
– preoccupation with self and appearance
– substance abuse issues
– inappropriate risk taking, impulse-control and lack of inhibition
– social awareness and invasive behaviour
– delusions, hallucinations, and excessive internal dialogue.
Enjoyable Treatment Process
Neurofeedback lets us train dysrythmic brain areas. Rather than engaging the conscious mind, which slows us down, we are training preconscious processes.
With sensors comfortably fitted to the brain areas we want to train, we detect brainwave patterns real-time while watching a movie. When these patterns are inefficient, the volume drops momentarily. This is the feedback we are giving our brain, it is solely auditory or visual, and the sensors are for measurement only.
The brain area we are training recognises this – while our conscious mind is focussed on the movie – and adjusts its behaviour to restore the normal volume. With repetition, throughout a session, learning occurs.
Meanwhile our conscious mind is solely focussed on the film showing on the screen; the training process is passive in this sense and all that is required of the person is to be engaged by the movie of choice.
Sessions can last from fifteen minutes to over two hours when tolerated. We generally achieve substantial calming in session that make previously unthought of film durations now attainable.
Intrusive Thoughts
Self-criticism overshadows motivation and confidence, and we become self-aware and distracted by negative thoughts and feelings. Some use acquired habits to distract from this. Our confidence, motivation and social interaction suffer as a result.
One recent explanation for intrusive thoughts is sleep deprivation, specifically REM sleep, and resultant inability to downregulate unwanted memories. Another source can be excessive higher frequency brain activity, resulting in distracting internal dialogue. Both have neural correlates which we can detect, and address with neurofeedback training.
Obsessive checking behaviour and compulsive ordering, washing and hoarding can be manifestations of this process. Both phenomena have neural correlates, which we can identify with a brain map, and train accordingly with neurofeedback.

With a brain map, we can identify vulnerability to various mechanisms of self-deprecation, ranging from thought, habits and mood regulation to actions and self-acceptance. With neurofeedback, we train core networks responsible for our sense of self, as well as brain areas related to adverse behaviour and sensory interpretation.
Clients report feeling more grounded, calm and optimistic. Neurofeedback takes a holistic approach, and we are usually also working on areas related to productivity and motivation.
Intrusive thoughts can have differing origins, or can relate to various neural phenomena. For example, there is the frequent initiation of rituals as a result of over-monitoring consequences of actions (“checking” behaviour). This occurs when prefrontal areas are overactive. Internal chatter is a different, and possibliy co-occurring symptom, whose vulnerability we can also detect.
Being stuck in a loop, detaching from the outside world, is a consequence of still other network flexibility impairments. Many overlap with schizophrenia and autism, and rather than diagnosis we are disaggregating the respective symptoms and providing a more granular view of neural correlates (neuromarkers) for behaviour patterns.
With neurofeedback, we can then train the respective brain areas to restore healthy functionality.
Comorbidities of OCD
OCD most commonly presents with a number of other mental health issues. With neurofeedback we can address most of these symptoms in an evidence-based, medication-free manner.
Around two-thirds of OCD sufferers also present with depression. One fifth have anxiety or panic disorder. Mood regulation, ADHD, trauma and substance abuse affects ten percent, as do body awareness disorders. Tics and autism can affect one in twenty.






Trauma and Neurofeedback - A Forward-Looking Approach
Trauma is fundamentally an inability to self-nurture – creating an emotional safe-space around us – and self-soothe – being able to talk ourselves down rationally from a situation. This can also manifest in dissociation and heightened pain perception, fibromyalgia and chronic fatigue. We ruminate about the past and worry about the future, instead of being able to enjoy the present.
Trauma and Anxiety are a result of inefficient sensory processing. We explain the scientific background and how neurofeedback training works in the following tabs:
(Scroll down on mobile)
Alpha Theta Neurofeedback Training
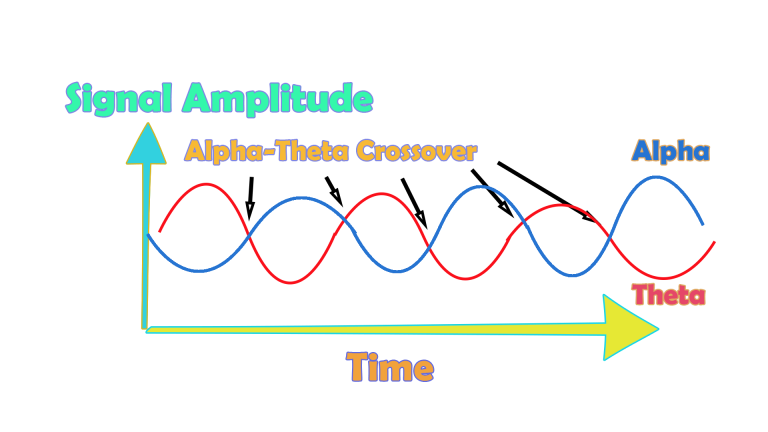
Alpha Theta neurofeedback training guides the brain through gentle oscillations between alpha and theta dominant states. The idea is that memories are accessed during theta dominance that can then be safely processed during alpha modulation.
Theta and alpha refer to different frequency bands of prevalent brain activity. When the slower, theta, is dominant, our brain is typically closer to sleep and our cortical activity is lower, in favour of more basic, sub-cortical structures. Alpha is a state of disconnected relaxation, and represents the core organisational frequency of our cortex. Each state activates a different part of the salience network, and reflects a mental transition between awake and pre-sleep, or shifting from extra- to intrapersonal based processing.
A session is usually thirty minutes, or multiples thereof, as the brain takes a few minutes to settle before commencing its alpha – theta modulation. The transitions between alpha and theta dominance are often visible on the EEG monitor, as they appear as ‘cross-overs’ every few minutes. Should a participant transition into actual sleep, delta activity will increase visibly. Sufficient mental calming before starting alpha theta training helps maximise training effects.
Alpha Theta training is done in a quiet room with minimal sensory input. The feedback is auditory, as two different but related soundscapes (e.g. waves vs. waterfall) smoothly transition, indicating to the brain which state is prevalent (alpha or theta). Participants describe the experience as intensely relaxing, sometimes emotional, and compare it to a power nap, feeling mentally and emotionally refreshed.
Neurofeedback Alpha-Theta training can be combined with guided imagery to address and process more complex, specific issues. It can also serve as a complement to cognitive psychotherapeutic approaches. Additionally, alpha-theta training has been shown to improve creativity and musical performance.
In preparation of Alpha Theta training, we recommend Personalised Brain Training based on a qEEG brain map.
Self-Regulation and the Brain
Trauma and anxiety cloud our perception and curtail a positive outlook. We discuss the various manifestations of each lower down this page.
Left untreated, a negative feedback loop can ensue: We lose synchrony with our environment, resulting in reduced drive, motivation, activity, interaction, recuperation (sleep) and functionality. What’s more, this traps us in a cycle that makes effective social contact more difficult, and thus deprives us of further options.
Trauma and Anxiety are a result of inefficient sensory processing. The understanding of our environment which we obtain from our senses does not relate to that experienced by others. We become unable to synchronise and share a reality, a core requirement for human interaction. It is a road to isolation, in particular perceived solitude.
Perception and emotional response start in the head, though their manifestations can quickly become physical. Pain perception has clear neural correlates. Our brain controls our Autonomous Nervous system, and hence our physiological tone and flexibility.
With a Kaiser Neuromap we can identify dysrhythmia of relevant brain areas, both emotional and physical, and then train these with neurofeedback.
We are restoring the brain’s ability to digest past events, look positively into the future and engage effectively in the present. It is a forward-looking approach that is also holistic – as well as training brain areas responsible for arousal, mood and vigilance, we restore focus, drive and motivation, thus restoring self-confidence in a multi-faceted way.

Our autonomic nervous system is primed to produce sympathetic nervous system responses, or fight-flight-freeze mode. This wears us down, as it is more energy intensive, our recuperation periods are shortened and we can even become used to the adrenalinergic buzz of being in hypervigilant overdrive. It becomes a safe space. Our pain perception is altered and fluctuates between numbness and hypersensitivity. Deprived of a ‘calm’ reference state, we become vulnerable to overattributing emotions to sensations.
Dissociation is another phenomenon that can ensue, and this can be subtle and paroxysmal. Engagement of defensive mechanisms is triggered pre-, or subconsciously. This can compromise our ability to rationally self-soothe – the role of our prefrontal cortex. Instead, our limbic system is primed. We also lose our emotional sense of safety. The integrity of our Default Mode Network is challenged, as is the natural transition between its activation and that of the Task Positive Network. We are less able to regulate engagement with our environment and the neurological basis for our sense of self is under threat.
There are distinct brain areas regulating pain, physical sensations and our self-awareness, and we can train these with neurofeedback. We can also train brain areas with strong connections to sub-cortical structures that regulate our autonomic nervous system, including the amygdala and our reticular activating (or limbic) system. Our brain is ultimately in charge of trauma response, and with neurofeedback we can assess vulnerability to its various submodalities, and address these with training. This is evidence-based and effective.
Trauma Symptoms
Trauma is essentially when we’re not expanding – when we are restrained in our ability to unfold our personality, ambitions and realise our dreams.
This can be precipitated by specific events, or an aggregation of contributing factors to our inability to self-nurture.
Our ability to find emotional security becomes impaired, and we begin to worry about the future, ruminate about the past. We become subtly detached from the moment and its meaning. This is the beginning of mental health issues.
Alpha Theta training provides a way of gently returning the brain from certain patterns of dissociation and process these with appropriate detachment and rationale. Neurofeedback training then helps the brain to restore functionality and resolve these in a forward-looking manner. We recommend ongoing neurofeedback training with alpha theta training.
The first indication that we are experiencing trauma / PTSD is when we find ourselves not living in the present. Enjoyment of the moment and social interaction is clouded by constant ruminations about the past, and worries about the future. We are unable to ‘let go’, relax, and grasp opportunities as they present themselves in the Now.
We are plagued by intrusive thoughts that bring us back to events in the past, which needn’t even be related to a traumatic event, but which remind us of some inadequacy and amplify our self-doubt. Feelings of shame and guilt come into the picture as well, further eroding our self-confidence. “How can I be happy and enjoy this after what has happened?”. Similarly, our perception of the future is shrouded in worry and fearful anticipation. Uncertainty is our greatest foe, our perception of safety is unhinged by any doubt as to what could happen next.
The absence of a plan becomes a concern, the lack of clarity as to what’s around the corner a burden. Negativity associated with the past deprives us of hope. We are thus unable to see uncharted territories ahead as an opportunity, and much rather dwell on impending threats.
Indeed, our system is primed to protect us, and we are in survival mode. This process becomes self-feeding as we become addicted to the hyper-arousal our sense of fear induces. Our sense of joy and looking forward to fun becomes clouded to the extent we forget and no longer yearn it. Detachment sets in, further isolating us from feelings that previously motivated us. This process can even start slow and subtly, yet the cycle is self-fulfilling and deprives us of the necessary perspective to break and get out.
In Personalised Brain Training, our definition of trauma is wider. We include for example perceived loss of social standing, which can be either the cause or the consequence of a traumatic event or development. The perceived loss of social position results in us feeling judged. We become hypersensitive to how people approach us, talk to us, deal with us.
This is a subjective concept, as it should be, given that trauma should be recognised as an issue of perception by the affected person, rather than a concept being ‘awarded’ by an unrelated party, though external affirmation can help and medical advice should be sought in any event. As humans, social recognition is a critical component of our biological drive to propagate. Attraction relies on this, which ultimately leads to bonding.
Consequently, there are numerous brain areas devoted to, or involved in, the assessment of our position with regard to others. When our self-perception is assailed, or even the viability of our self is questioned, we are naturally shaken. Various brain areas become dysrhythmic. These include areas responsible for our body control and awareness, and many therapies focus on engaging the body and somatosensory system with a view to inducing cerebral changes.
However, this is only a part of the picture – there are many, arguably more powerful neuronal centres in the brain that are affected by trauma, and with a Kaiser Neuromap and Default Network Training (together, Personalised Brain Training), we can assess the issues more accurately, completely and efficiently, as well as then successfully training the brain to overcome trauma and setting ourselves on course for a positive trajectory.
Another consequence of trauma is that we may feel unable to rationally assert a sense of safety. This is different to self-nurture, or an emotional sense of safety. When we are unable to talk ourselves down from a situation we lose the ability to effectively regulate our moods, to switch off when we need to, and ultimately can become excessively paranoid.
There are neural correlates for this behaviour, and we can asses this with a Kaiser Neuromap. Safety and assurance are core needs we are programmed to seek to fulfil. Authority and role models help us in this quest. When we become dysregulated in our ability to self-soothe, we are also compromised in our ability to find paternal guidance. As a result, we tend to over-idolise figures who seemingly exude strength and power, or disobey completely and become unnecessarily rebellious – both immature behaviour patterns. Resetting this balance is crucial to achieving calming, regulated emotions, reduced hypervigilance and controlling impulsiveness. Personalised Brain Training lets us achieve this.
When hypervigilance persists untreated, we face further problems.
Physically, our heart beats faster and harder, more of the time, which is a clear stress on our system.
Mentally, we become prone to developing intrusive thoughts, even when we are able to relax, and more so when we are stressed, where these can take on third-person character, a voice in our head. This can have a destabilising effect, not least because we are now spending energy ‘defeating’ other perspectives we are internally engaged with, and thus distracting us from the ‘now’. Being on hyper-alert can also make us more susceptible to feeling relational to sensory input, in that we feel that everything is directed at us, which can set us up for psychosis.
As we lose our ability to enjoy the moment, our social interactions suffer. Exercising our social brain keeps us alive and forms the basis for sound mental health. Our brains are adaptive, and we need to provide stimulus to maintain connections and sustain flexibility. Isolation deprives us of many necessary exercises. For example, brain areas that deal with face recognition also respond to affective interactions and the ability to discriminate between emotional content of faces. We need to keep training these brain areas through social interaction in order to maintain emotional recognition – it is not a surprise that perpetual mask-wearing heightens our social anxiety (aside from adverse physical effects).
Social recognition, a key component of our biological need to attract and bond, is driven by sensory interpretations. Again, we need to exercise brain areas that contribute to this, including language and speech generation and comprehension, auditory sensitivity, and monitoring rewards for actions, both directly and vicariously. Our mirror neuron system contributes towards learning from others’ mistakes or examples, and consequently the storage of social rules necessary for constructive functioning in a society.
Inclusion is imperative to establishing a healthy self-image or sense of self. This in turn is crucial to forming stable relationships with friends, family and forming healthy alliances necessary for personal and professional progression. When we lose our sense of belonging to a group or cause, we may become unstable in our self-perception and our relationships with others. The effect may snowball into perceptions of abandonment, feelings of emptiness and dissociation; this in turn correlates with mood dysregulation, impulsive and often dangerous behaviours, intrusive thoughts and potential self-harm.
With Personalised Brain Training, we can assess vulnerability to these traits as they manifest in functional brain area dysrhythmia that shows in a Kaiser Neuromap; with Default Network Training, an advanced form of neurofeedback, we can train these brain areas and networks in a holistic manner to help re-establish balance. This enables us to reconnect with our environment and re-enter a positive feedback loop.
Sleep is adversely affected by trauma. First, the mind needs to ‘let go’ in order to enter deeper sleep cycles, which is a challenge for many. Excessive rumination and intrusive thoughts can hinder this, as does the loss of our ability to rationally calm ourselves down. The depth of our sleep is governed by our ability to self-nurture and create an emotional ‘safe space’. Homeostasis during various sleep stages is governed by other parts of our brain, some still involving the cortex. With a Kaiser Neuromap we can detect dysrhythmia in the relevant brain areas and train these accordingly with Default Network Training (together, Personalised Brain Training).
Focus and organisation suffers as a consequence of sleep issues. This time, different brain areas are affected, which we can also train. When we are unable to concentrate and produce our best output, we become demotivated and our mood and sense of self suffer. Again, there are brain areas responsible for these aspects of being, for which we can again detect dysrhythmia and provide neurofeedback training. The process is holistic – many components have to work together effectively for us to function optimally.
Mood regulation suffers when we lose social integration, sleep and focus. Neurofeedback training found to significantly help 80% of people with depression by aiming to restore motivation, improving sleep and focus, and reducing anxiety.
There are numerous potential cortical contributors to depression, and with a brain map we can see vulnerabilities.
Neurofeedback training lets us address these as well as establish a generally improved sense of well-being in a holistic manner. he positive effects of neurofeedback training have been shown to be lasting. Neurofeedback is non-invasive and medication-free.
There are multiple types of anxiety, each correlating with one or more brain areas being dysrhythmic:
- Social anxiety: When we’re in a situation with other people and our understanding of the social dynamics and complexities is overwhelmed.
- Sensory overload: our brain interprets all sensory stimulus as directed to ourselves. We lose the ability to discern what is directed at us, and which matters or interactions are of no concern to us. This sets us up for panic attacks and ultimately psychosis. It also means we become singular in our perspective, unable to take on other points of view
- Loss of narrative: Our episodic understanding of the situation, how we got there and what happens next, is impaired, and we are unsure of where we are and where we’re going. This hyperactivates our amygdala, and the sensation is highly emotional
- Auditory sensitivity: we become prone to overly interpreting the emotional content of words and sounds, creating an air of prickliness and pushing people away without knowing it
- Activation: Our ARAS is responsible for setting the right level of physiological arousal, or wakefulness, for the situation, and to remain stable there. When this is on overdrive, we are pushed further into fight-or-flight mode than necessary, thus heightening sensory sensitivity. Panic attacks are an extreme manifestation.
- Trauma: an inability to self-nurture – creating an emotional safe-space around us – and self-soothe – being able to talk ourselves down rationally from a situation, thus resulting in mood instability. This can also manifest in dissociation and heightened pain perception. We ruminate about the past and worry about the future, instead of being able to enjoy the present.
- Intrusive thoughts: Self-criticism overshadows motivation and confidence, and we become self-aware and distracted by negative thoughts and feelings. Some use acquired habits to distract from this. Our confidence, motivation and social interaction suffer as a result.
The primary issue of trauma affects brain areas that are activated during empathy and forgiveness. With these two qualities impaired, our emotional life suffers, as do our social capacities. With neurofeedback training, we can restore functionality of these brain areas. Another reason this is important is because we do not want to become oppressors ourselves. As we lose our sense of emotional investment in our surroundings, we become careless with regard to others’ feelings and needs.
Implicitly, we are now capable of unintended yet real behaviour patterns that can harm others, as we become deaf to feedback. Not only has trauma affected us, it now makes us perpetrators that pass it on.
Besides reduced social interaction and a less meaningful emotional life that is now more self-centred – and with the wrong type of therapy, becomes self-indulgent and self-perpetuating – we can experience a physical withdrawal from our environment. Dissociation can be momentary and intense, or subtle and ongoing to the extent that we are not even cognisant of it. Either way, our bodies retreat from sensations, analogous to our emotional withdrawal.
Many therapies aim to revive our sense of ownership of our bodies, and thus ultimately our life and future, by training our body awareness in various ways. Realising that our bodies are steered by our mind, specifically our cortex, we can train the relevant brain areas that govern our body perception and movement execution.
Neurofeedback training effectively complements these approaches by directly treating the areas involved in perception and interaction with our surroundings.
One of the first manifestations of trauma is in our bodies. Aside from heightened physiological arousal, a form of paralysis can override our natural motions and postures. Stress, and pain ensue, which can often be felt all around the body. Fibromyalgia is a variant of this phenomenon, as are headaches, chest pains, and chronic fatigue.
There are many techniques for combating this form of physical dissociation. Neurofeedback complements these by training the brain areas that instruct the body to behave in this undesirable way. It is a holistic approach, and we restore overall calming while providing the brain with rational and emotional capacity to overcome its challenges.
Trauma and Empathy, Forgiveness
A brain area directly affected by Trauma happens to govern our ability to empathise, as well as our capacity to forgive.
Importantly, this is borne out of physiology – the physical reality of bodily functions (in this case, the brain) controlling our personal and social functioning. This is different to, say, psychology, which attempts to model behaviour patterns and their linkages, on a more academic, and hence detached, level. Physiology is real. We can observe the relationship between social and emotional conduct and the activity of specific brain areas, and there are over 200 such studies conducted annually.
When brain areas become dysrhythmic, such as through the impact of perceived trauma, their ability to direct other aspects of our being and interaction can become impaired. As a result, we can observe how a person’s scope for internalising other’s emotional state is reduced. The ability to forgive, overcome judgements and move on, is similarly compromised.
An example of how being traumatised may impair one’s ability to show empathy and forgiveness, or emotional insight and compassion, is possibly the story of Bessel van der Kolk, author of “The Body Keeps the Score”. The author of this popular book examining the physiology of trauma, which notably ends with a chapter on Neurofeedback, was himself fired from his own trauma centre, by another entity. A 2018 Boston Globe article asserts that he was “fired from his job over allegations that he bullied and denigrated employees at his renowned Trauma Center”, though this should not be confused with allegations against another director at around the same time “for violating the code of conduct in his treatment of women”. Arguably, an involuntary, surprising exit from a place of work he contributed towards for 35 years could be seen as a traumatising event. An apology letter by Bessel van der Kolk on his own website has been extensively analysed – see “The Anatomy of an Apology”.
On a mission to “better understand and treat the evergrowing number of trauma victims produced by this harsh and violent world of ours”, it seems clear that Bessel van der Kolk has grown from the experience of being a victim. Formulations such as “the vast majority .. did not experience me in this way” and “we have negotiated a settlement” might leave some readers to question whether there was ever a possibility that someone in his organisation felt accordingly victimised. We now have the concept of “pernicious” victims, which appears to be an oxymoron – did they even exist? If not, why settle? With whom? Either the ostensible victims have not been able to forgive, or Bessel van der Kolk – himself a perceived victim – has not forgiven his accusers, or indeed both.
We hope that Bessel van der Kolk’s tour de force continues to dispel any doubt and evil, while extending appropriate sympathy to victims (should these have ever existed).
Having been traumatised by this experience, Bessel van der Kolk certainly appears to see himself as a victim. His reactions show how important empathy for victims, and forgiveness is.
Perhaps another corollary is that trauma can be a perception issue, and attempts to formulate this into reality may create perpetrators out of self-perceived victims.
In this letter, Bessel van der Kolk appears to give some credence to the possibility that some victims could have felt this way about some occasions of his alleged behaviour. In it, he appears to provide ‘little’ insight into how this could have arisen, while partially acknowledging its credibility (“such accusations cannot be entirely pulled out of thin air”).
A compassionate insight into the reasons why alleged victims find it difficult to confront the alleged perpetrators appears to be lacking (though his own book suggests that trauma results in suppression and an inability to confront the event, or its memory).
A 2018 article quotes him addressing power imbalances in the workplace, indicating a virtuous transformation: “That is a reality. I’ve grown up in the medical world, and people have said all kinds of things, like, ‘If you ever do this again, I’ll fire you,’ and ‘I will not promote you unless you do this…’ You just suck it up. Certainly, when I first started the trauma center a long time ago and came from that world, I thought that was sort of OK. But very quickly my colleagues said, ‘No, we don’t do it that way. So I learned I should not adopt the model I was trained in in medicine.”
Two years on, in 2020, a legal resolution seems to have been reached, involving an undisclosed settlement, and Bessel van der Kolk explains the situation, confirming that the allegations of “denigration” and “bullying” were “pernicious”. He humbly adds that “while I’m deeply committed to be kind and empathetic, I am also aware that, in times of stress, there is room for me to improve my interpersonal sensitivity”, noting that “the vast majority of persons with whom I have worked for forty years did not experience me in this way”.
Excerpts from Bessel van der Kolk’s letter to his colleagues, that had been placed publicly on what appears to have been his website with an invitation to share:
“Dear Trauma Center colleagues,
As you can imagine, I am devastated reading the allegations in the Boston Globe that I have been bullying and denigrating my colleagues at the Trauma Center.
I am also aware that such accusations cannot be entirely pulled out thin air, and that some of you may have felt hurt by me, even though none of you have ever confronted me with such misbehavior. If I have inadvertently denigrated or bullied any of you,I would like to know about it, apologize and make amends.
As you know., I am a strong believer in doing your own personal work, and in my book, the Body keeps the Score, I describe some of that journey for myself,.
If you do not feel that Andy Pond’s insinuations represent reality, I hope you will be vocal and public about how you feel about character assassination, and speak your truth.
Thank you, and I hope to see you all under better circumstances.
Devastatedly yours,
Bessel
Feel free to share.
Bessel van der Kolk MD
Medical Director Trauma Center
Professor of Psychiatry
Boston University School of Medicine”
Note that different versions of this letter exist, though with substantial similarities. A Facebook page created during the year of launch of “The Body Keeps the Score” (2014) has a post from 10 March 2018. To our knowledge, the existence of such letter has not been refuted, and the Facebook page still stands, whereas the URLs www.besselvanderkolk.net and www.besselvanderkolk.com appear linked, according to various searches into their history. Should such relationship never have existed, the Facebook page fake, the letter (in any permutation) not have existed, this should be made clear such that such impression is not reasonably created, and we would look forward to supporting Bessel van der Kolk in clearing up such needless confusion.
In summary, trauma has a physical effect, and by addressing its physiology, we can help healing. Neurofeedback provides such a method, as is evidence-based, confirmed both by science and popular literature.
Traumatic experiences undoubtedly affect our current behaviour, and as a result, how we shape our future.
A reduced capacity for empathy and forgiveness is one such example, as described above.
Memory of traumatic events is embedded in our physiology. By this we mean that memory is synaptic, that is, a biological phenomenon. We have known this since the 1950s, from the case of “patient H.M.” – probably the most studied person in the history of neuroscience. This patient was able to access old memories while being unable to form new ones following an operation that removed part of his hippocampus as a treatment to relieve seizures. A new level of complexity in the process of memory formation by the brain was thus discovered.
There are different parts of the human brain that store, and recover memories of events. Narrative, or declarative memory, involves many cortical areas. Conditioned responses, such as physical reactions learned during situations that put our very existence to test, i.e. trauma, are often not associated with conscious recovery of the event that spawned them. Learning in this case involves sub-cortical structures, and their recall might only have physical manifestations, such as changes in physiological arousal that appear disproportionate, and as such confusing given the lack of accompanying narrative. These can include sudden intense feelings, sensory processes, avoidant behaviours and even flashbacks and dreams. Seemingly irrational due to a lack of associated narrative, they are still ‘held’ within our brain.
These forms of conditioning can interfere adversely with our everyday lives in many ways. Some forms of therapy focus on the physical manifestations, in effect retraining our brain by expanding its flexibility to induce calmer, more rational or appropriate physical and physiological behaviour. Yoga, breathing exercises, team sports, singing, dancing, acting and music production are some of these.
Neurofeedback provides us with a complementary approach to help the brain achieve better flexibility.
There is considerable doubt as to the validity of repressed memories. Accessing these through interventions, in their various guises, has been shown to be a controversial endeavour in many cases.
An example of this is the story of Patricia Burgus, whose postnatal depression was diagnosed as a multiple personality disorder. Subsequent therapy utilised multiple ways of ‘accessing’ her repressed memories, with the result of unearthing satanic cults, expanding her perceived number of personalities from 20 to 300, and withdrawing her children from her care in placed into a psychiatric hospital.
Cases such as these tested the reliability of the interventions used in the 1980s and 90s, and saw a subsequent reversal in this trend.
Neurofeedback provides us with a complementary approach to help the brain achieve better flexibility.
Neurofeedback lets us train dysrythmic brain areas. Rather than engaging the conscious mind, which slows us down, we are training preconscious processes.
With sensors comfortably fitted to the brain areas we want to train, we detect brainwave patterns real-time while watching a movie. When these patterns are inefficient, the volume drops momentarily. This is the feedback we are giving our brain, it is solely auditory or visual, and the sensors are for measurement only.
The brain area we are training recognises this – while our conscious mind is focussed on the movie – and adjusts its behaviour to restore the normal volume. With repetition, throughout a session, learning occurs.
Meanwhile our conscious mind is solely focussed on the film showing on the screen; the training process is passive in this sense and all that is required of the person is to be engaged by the movie of choice.
Sessions can last from fifteen minutes to over two hours when tolerated. We generally achieve substantial calming in session that make previously unthought of film durations now attainable.
Personalised Brain Training is Forward-Looking
Trauma is a debilitating, negative state, both mentally and physically. Unresolved, we risk becoming desensitised, unempathetic and destructive, even possibly turning into abusers ourselves.
What’s more, many approaches to dealing with trauma are themselves riddled with self-indulgence and self-interest on the part of the provider – there is no end to disappointments and betrayals that can be unearthed in a person’s history, and unsurprisingly many psychotherapy approaches are lengthy and possibly self-reinforcing (re-traumatising). As a participant in such programmes, we are prone to developing our identity around our ‘trauma’, not least due to the time spent analysing this.
Personalised Brain Training takes a forward-looking approach to overcoming our current situation. It aims to restore functionality and positive feedback loops in the shortest possible time, without indulging in recollections of the past nor medicinal numbing. The future starts in the present, and neurofeedback training is for persons who actually want to get better and are willing to manifest their thoughts accordingly, with the help that brain training provides.
Neurofeedback for trauma and PTSD is evidence-based, effective, non-invasive and medication-free.

Every person is different and has a unique way of responding to being shaken out of their perceived safety. A brain map shows us which brain areas have become dysregulated, and we then train these with neurofeedback. We use David Kaiser’s Default Network Training, which is an advanced method superseding the Othmer Method / ILF. Training the brain this way shows it what it it’s like to be functional again, over it, able to get on with it. With practice we become able to reform our trajectory and regain a sustainable, self-reinforcing, positive environment.
As a result, we are no longer trapped in the recursive, debilitating loop of intrusive thoughts, avoidance behaviour and negativity. Instead we are able to live a positive, constructive and productive life while viewing our previous ‘hole’ with healthy detachment and self-forgiveness.
Many symptoms of OCD, aside from checking behaviour and compulsive ordering, are found in the form of cognitive distortions as classified in the Cognitive Behaviour Therapy approach. Each has neural correlates, and with a brain map we can detect which are vulnerabilities, and then train these with neurofeedback. This process works with the subconscious, or preconscious mind, and does not depend on talk therapy and other methods aimed at our conscious mind portal. With neurofeedback, we are equipping the brain with the ability to take on new perspectives, and practice more efficient behaviour. Neurofeedback training works well in preparation for or in conjuction with CBT in our experience, providing the neural groundwork for better learning of efficient behaviour, improving sense of self and making environmental changes that produce lasting effects.
Many of the fifteen core cognitive distortions summarised by Burns in 1980, and which form the basis of CBT symptom analysis, can be grouped as a result of their common neural correlates, that is, specific brain areas or networks that are likely dysrythmic for this behaviour to occur repeatedly.
In the first instance, we have relational thinking, which is when we find that all sensory stimulus is directed at us, we are at the centre of every situation, our perspective is narrow and rigid, and we are incapable of self-insight and change. This can be an acute anxiety by itself, and the source of deep depression. It also makes us inefficient in our social interaction, partly because we cannot filter and ignore irrelevant stimulus, and also because it causes friction with others of different views and perspectives. We tend to overgeneralise, catastrophise, personalise, seek control, be righteous and inflexible, and expect things from others and the universe in general while applying different standards to ourselves. One or more of these can be applicable, and they are usually the primary result of relational thinking, a vulnerability that is easily identifiable on a brain map and has scientific underpinnings (fMRI studies). Some of this behaviour can be coupled with impulsiveness, disinhibition and weak social boundaries, meaning we are quick to apply judgement, blame, expectations and control on others. We might also be prone to polarised, or black&white thinking, showing low appreciation for complexity or nuance.
Another set of attributes is based on our ability to self-nurture, and to feel part of and accepted by some bigger cause or group. Without this, we are quick to change direction and judgment, tending to extremes. We might also be quick to blame others for our own shortcomings and apply different standards to ourselves. This is also a contributor to polarised thinking patterns and control fallacies.
Also, our ability to self-soothe impacts our sense of fairness, as well as appropriate inhibition. This is governed by specific brain areas, which we can train to improve mood control, the ability to fall asleep, and to be in control of our urges.
Our Default Mode Network is our neural representation of self, and its integrity relates to our feeling of groundedness, self-acceptance and flexibility. Training this with Personalised Brain Training helps us achieve lasting results on a stronger foundation.
OCD and Cognitive Distortions
Case Studies
Deirdre’s daughter Monica, 10, suffered from severe intractable epilepsy, with up to twenty awakenings due to heavy seizures in a night. While working with Monica, we also did neurofeedback training with Deirdre. Effectively in a state of constant alert and hypervigilance, Deirdre had a strong grounded personality, which showed in her brain map. Nevertheless, the physical and emotional strain was taking its toll, in particular on her sleep, and consequently her ability to focus on her writing project, while managing an impending divorce and relocation. Within the first sessions, her sleep improved substantially and she felt more productive.
"I felt so calm last night! And slept like there were magnets between me and the bed. 10 hours straight."
"Slept like a log."
"Since I started neurofeedback training, my dreams have come back!"
Client testimony.
Lorna had enjoyed what from the outside appeared to have been a privileged life, having enjoyed private education, a lucrative and indeed fulfilling role in the family business, and accumulated some reserves. She had been medicated for bipolar disorder and ADHD from the age of eight, in what she felt was a suppression of her bubbly personality that didn’t conform to parental expectations of ‘order’ or ‘normal’ behaviour. She had always been social and outgoing, enjoyed boarding school, yet she now felt things had come to a head and that she was not living to be the person she could be. Instead, she believed she had conformed to the wishes of her family and ignored her own needs, emotionally, socially, and fundamentally with regard to her identity. Mood swings, disturbed sleep, lack of focus and self-critical thoughts deprived her of joy in her life. As opposed to deprivation of nurture, Lorna had been domineered by her parents, and not been able to develop her own sense of self-nurture. Her identity and sense of self worth were shattered.
Within five sessions, Lorna’s sleep improved noticeably, as did her energy and motivation. She enjoyed doing long sessions, in particular the film “Now, Voyager” with Bette Davis reminded her of her upbringing and situation. After ten sessions, Lorna began working with a talk therapist to reorganise her life and ambitions – teaching in India was a dream she thought could be realised. Her sense of despair had disappeared, and yielded to a slightly overly self-conscious anxiety, which was the first step past numbness. Lorna’s productivity improved and she began to set herself higher goals, leading to some frustration, yet this substantially contrasted with her previous despondency. A further few sessions helped with the self-blame and internal chatter, and Lorna is on a good trajectory.
Maria, 77, an avid reader, discovered in her 60s that she had an irreversible eye condition, a glaucoma, that was causing her tunnel vision. She was able to stabilise the development with medication, yet it led to a few nasty falls, one of which left her concussed. A Kaiser Neuromap showed the expected areas of brain hypometabolism, and we trained her accordingly. Ten sessions later, her sleep was restored, as was her perceived memory, and a remap showed that the brain areas had responded. She felt more productive and grounded and enjoyed the experience of watching multiple movies, her favourite being with Audrey Hepburn.
Marcus’s wife had suspected that certain of his mannerisms had changed, he had become more impulsively aggressive at minor things that changed his routine, and she believed his gait had changed, beyond the mere effects of working from home for the last, stressful, two years. Socially withdrawn, Marcus was focused on his consulting work which had started to pick up again. The joy in his life was lacking, despite having a supportive family.
A brain map revealed some unusual areas of hypometabolism, that would warrant further investigation into whether they are early signs of neurodegeneration, possibly Alzheimer’s Disease. There are certain non-specific neuromarkers, as well as expected reduction in functional connectivity of the corpus callosum that joins the two brain hemispheres. We also found signs of emotional stress and a tendency to internalise, and excessively blame oneself. Two neurofeedback sessions based on these findings returned Marcus’s sleep to a level he had forgotten existed. He became more focused on his work and related social interactions, and had the best financial year of his career.

Linda had been betrayed by her husband. The realisation set in just before her fiftieth birthday. In her second marriage, living in her dream house with an eleven year-old daughter, she felt vulnerable and despaired. They had gotten through the lockdowns as a family, while her social life suffered, and she no longer felt her bubbly self. On top of this she was going through menopause, a disorienting experience, and her daughter was striving for teenage independence in a most hurtful way. Linda had experienced depression before, tried every medical and alternative healing path, and even been to rehabilitation as a way of setting a line to her partying lifestyle in her twenties (“rehab doesn’t work. I’ve made great friends there though!”). She knew there was a resilience in her, which after all had enabled her to transition from being a single mother with an insecure singing career to affording her current lifestyle and the stability it represented. This was now shaken.
Self-doubt and introversion were not her natural habitat, yet she felt isolated, and even began to think she had incurred brain damage as a result of her youthful excesses. Linda was taking anti-depressants and immersed herself in a temporary sales role, which had just come to an end. With time on her hands, she decided to try neurofeedback training.
Visibly nervous excitement before the first session quickly subsided. We started with a brain map, and just wearing the shower cap-like recording device made her feel calm and sleepy. This takes about half an hour, and we quickly proceeded to do a first training session. The cap is replaced with three sensors gently fitted to her head at the areas we look to train. Settling for a Robert de Niro film, Linda was quickly immersed, relaxed and amused. The morning passed swiftly and she was on her feet ready to pick her daughter up for school after the session ended. She noted that her sleep was particularly deep that night.
Linda’s brain map showed substantial deactivation of her prefrontal cortex, something she worried was a result of historic substance abuse. A remap after ten sessions showed visible improvements on this metric, as encouraging as her other improvements in mood, focus and self-confidence.
Intrusive, self-critical thoughts subsided and her motivation returned along with focus and deliberation. She felt particularly productive after each session, and this gave her great confidence. Changes were apparent in every way. Even her husband was amazed – “you’re back to your bubbly self!” Linda began feeling a healthy sense of detachment, and was no longer lifting the weight of the world by herself. She had gone from being reactive and despondent to taking control and setting the rules, which her husband obligingly acquiesced to.
A former singer in a band, she started humming tunes to herself again, and there was music playing in the house, replacing the solemn silence that was deafening upon our first meeting. Soon, projects began, she replaced artwork in the living room and began some redecorations.
Being on her own was no longer her refuge of choice; instead she rekindled productive relationships, and set aside people and places that were soaking up her energy. Her schedule filled, as she accomplished her spinning workouts before our sessions, and project partners were waiting outside as we finished.
Linda started to accept her marital situation, redeemed her sense of self-worth, and found a way to make partnership and parenthood work beyond traditional confines.
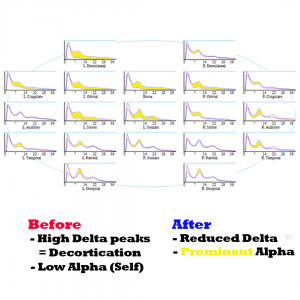
Her brain map corroborates the transition: previously absent alpha peaks emerged visibly, mirroring the cognitive resuscitation she was experiencing. Other vulnerabilities in her initial brain map included:
- mood control;
- lack of emotional safety, or feeling ‘underloved’, both by family and the world at large;
- heightened auditory sensitivity and a tendency to over-attribute emotional content into how things are said;
- focus and planning issues;
- various anxieties – “what’s next”, social anxiety, a sense of everything being directed at her, hypervigilance, and emotional betrayal
- disengagement from her surroundings.
Linda did twenty neurofeedback sessions, over the course of seven weeks, usually three per week. During this time, she had dropped the use of anti-depressant medication (in consultation with her prescribing GP / medical doctor). We did a remap after ten sessions, which showed substantial changes in her overall brain activation and guided the next ten sessions. (She had already commented, “It’s worth it!” after session five). After twenty sessions, Linda’s perceived transformation was corroborated by her final brain map. Of particular note is the way her immediate family embraced the changes, as her daughter began confiding in her.
Anna was prone to strong intra-day mood swings as well as having endured a manic episode, during which she became the subject of financial and emotional exploitation. Importantly, Anna was not psychotic; however she suffered from strong attachment disorder, fear of abandonment, some social awkwardness as a result of an impaired sense of self, and lack of ability to rationalise emotions, despite her warm demeanour.
Following a particular slump triggered by betrayal, and being subject to physical violence, she began neurofeedback sessions. Her sleep improved immediately, as did her outlook. Within five sessions, she had become her usual optimistic self again, and began looking for a new vocation. Within weeks, she had a new job that combined two of her passions and talents, and on a solid path to recovery and forgiveness.
Anna’s mood regulation has substantially improved during her ten overall sessions; she feels more grounded and motivated, while enjoying the cause of her work and the new people she is meeting.
Stephanie, 40, had recently suffered numerous destabilising incidents and conditions that deprived her of her joy of life and made everything seem extremely stressful. One night while preparing dinner, a confluence of her husband’s criticism, her kids screaming and the music on the radio overloaded her senses and she smashed a plate in desparate frustration. It was as if everything was directed at her, and her mood swings and lack of emotional support exacerbated the erosion of purpose she had come to feel. The previous years had deprived her of both parents, and she had ceded freelance work to raising her small children and looking after her ailing mother. Next-door building work continued throughout lockdown, and the family was on the constant verge of deciding to move. Furniture and clothes were packed, and the idea of nesting could not seem more remote. Stephanie felt under constant assault while not progressing personally or professionally. This strain entered her previously strong relationship with her husband, himself under substantial work pressure. Having self-diagnosed as PTSD, both decided to do twenty neurofeedback sessions.
Within a few sessions, Stephanie’s sleep was restored, and she became more motivated and relaxed. It no longer felt as though everything was directed at her, and she was able to respond to unexpected outcomes flexibly and with humour. This did wonders for her relationship, and she felt her children sensed this too. A brain map confirmed this progress.
Mary, 35, had contracted Covid in January and had almost been hospitalised. Six months later, she was still working part-time from home and felt like a shadow of her former self.
She was suffering from fatigue, anxiety and depression, and her sense of smell had not recovered. Brain fog, which could also be attributable to her perimenopausal stage, significantly reduced her productivity and confidence.
Mary’s sleep improved from the first neurofeedback session, as did her physical stamina.
Within three weeks, or five sessions, she noticed her sense of smell had begun to return.
Motivation and focus improved substantially through session ten. Mary felt reinvigorated and her self-critical thoughts subsided. “I’m there for my family again!” she commented.
We did another seven sessions, now spaced weekly, during which Mary remarked that she had never felt a clearer mind before.
It is not suggested that neurofeedback is a “cure” for issues arising from a Covid infection, and we will never know what caused her sense of smell to return. However it was reassuring to see how Mary’s general sense of self and well-being had improved during the time we were training.
Camilla had been diagnosed with anxiety, panic attacks, associated insomnia and mild depression. She was prescribed two anti-depressants – Mirtazapine and and SSRI – which she was able to reduce to a minimum dose over time. During the last three years however, she had six relapses, each following a similar pattern: Stress (emotional and work-related) and fatigue precipitated intrusive thoughts and worries, setting off a familiar path of insomnia; consequently higher anxiety, increased stress levels leading to panic attacks and depressive symptoms. The first few episodes were stabilised by resuming Mirtazapine, which helped restore sleep. The subsequent ones however failed to respond, taking months to stabilise sleep and reduce anxiety, which involved having to take time off work. In addition, she began to have somatisations, beginning in the spine and ultimately reaching her face. Migraines began to reappear when she became excessively tired.
Guided by a brain map, we began doing neurofeedback training twice a week. Camilla’s sleep became sound after the second session – “I feel pleasantly knocked out” – and she decided to reduce her Mirtazapine dose gradually in accordance with her prescribing GP. After eight sessions (four weeks) she was on the lowest dose, and even this left her feeling very groggy in the morning. Camilla had regained confidence in her ability to fall asleep, and stopped using Mirtazapine completely. Her anxiety levels were at their lowest, and she had began to work again, leaving a corporate environment to work with children in a mental health setting – a stressful yet engaging and meaningful activity. Her motivation had reached new levels, and she felt stable and confident, which showed in her stance and demeanour.
Ten sessions of neurofeedback training (each two hours) were sufficient to stabilise Camilla, restore her ability to sleep, and the confidence therein, as well as improving sense of self-worth, focus and motivation. She has not felt the need to use Mirtazapine again since.
Three months later, Camilla reports a major improvement in how she is able to set boundaries, both at work and in her personal life, and not neglecting her own well-being.
Janet, 56, was bursting in her every capacity – as mother of two teenage daughters, wife of a Long Covid-suffering income producer, daughter of an ailing mother with dementia, sister of a libertarian, care-free brother whose involvement with his kids contrasted starkly with her own, friend of contacts she had not had for three years since lockdowns, and undergoing her own menopausal transition.
She had spent the first term of the school year under severe stress, committing herself fully to support her two adolescent daughters, and inserting herself further into every fibre of their lives. She acknowledged that this was the reverse of how her brother was managing his children’s transition into early adulthood. Her own sleep had not been great to start the term with, and the built up worry, anxieties, and pre-existing mood control issues were exacerbated by the stress. Afraid of losing control, and the pending next stage of her own life once her children were going to go to university and leave the house, she compensated with surrendering any own motivations to perceived helpfulness and dedication.
Janet’s career as a casting director had been put on hold when she met her older husband John, whose banking career enabled them an adoption of two infant girls as she was infertile due to an autoimmune condition. In perceived competition with John’s two adult boys from a previous marriage, the girls were enlisted in the same schools. Insecurity and racism plagued their early upbringing, and they were now completing their Six Form (11-12th grade) in an acceptable private school. So big had the strain been on them, along with individual trauma, that both had mental health issues we resolved with neurofeedback training before and during term.
Janet had developed a paranoid cynicism that preceded all social interactions, as if to purposefully conjure up antagonistic reactions in an attempt to prove the worst and thereby achieve some sense of control and certainty. She was ever more convinced of intrinsic racism and antagonism towards any of her causes, and complained about the abolition of social distancing and other Covid measures that had happened over a year ago by now. Her overbearing intensity was difficult to dispute, and it appeared that her children, and husband, were suffering from her lack of self-insight. She would frequently break down when out of sight of her children, upset when her husband, himself suffering from Long Covid symptoms, found the occasional energy to call her ‘neurotic’. It would take a year after her daughters for her to commence neurofeedback training for herself.
Unlike her daughters, and her husband, Janet found it difficult to even tolerate opinions and views other than her own. Any perceived opposition, no matter how well-meant, would trigger her, and she had a tendency to infer the worst. Physiologically aroused, she would immediately turn combative and seek to quell any source of dissent or alternative point of view. This inflexibility applied to the most mundane of issues, such as changes in recreational plans for the day, to political views and current affairs, as well as deep-rooted convictions regarding the Covid pandemic and its resolution, which was being handled completely unsatisfactorily three years after the first lockdown. Janet’s autoimmune condition made her feel particularly vulnerable, and to her, masking and social distancing provided the minimum necessity in public interactions. She saw herself as the only agent of sense and pragmatism in her household, and therefore set the rules. The family was confined to isolation from the first lockdown. Physically, they were staying at home and not going to restaurants theatre shows as in the past. Socially, movements and interactions were severely constrained and limited to family outings. Meetings with friend were rare and heavily vetted, in particular with respect to Covid protocol observation but also perceived sense of responsibility. Volunteering projects, birthday parties and even cinema outings were off-limit. Living between two homes, both far from school and other classmates, furthered this separation. Her daughters were meanwhile the only ones in their class to wear N95 facemasks at all times – a condition that eventually got relaxed regarding outdoor breaks. Janet was driven by her perceived need to be involved and in control.
As a result, Janet was finding it difficult to feel part of something bigger – the outside world had firmly conspired against her, and from a neural perspective, this caused great instability. Her moods were also subject to violent, and fast, swings. Smiles and motivation could cede to despondence and crying in despair within a few hours. It was as if her fighting spirit was the only thing that could fire up her will power, at great emotional and energetic expense. Combat was her main driver, and she would find antagonism in anything and everyone, any fault triggering a polarised perception. School provided an outlet, as she got involved in every any aspect of her children’s education, trying to impose mask mandates there and actively communicating with teachers about coursework and teaching methods. Only parents with common grievances were part of her circle, and still this fluctuated by topic.
Unable to fall asleep easily, she would research the internet late into the night, and she was woken up easily at any time. Janet’s mind was racing at all times, and she felt like she was having to defeat internal voices of dissent when left to her own devices. She had long felt a dissociation from her body, and couldn’t remember the last time she had been given a hug. Her daughters’ growing desire for independence, and the prospect of complete solitude once they would graduate in a year’s time, frightened her. She was distrustful of medical doctors, especially as most had ceased to wear face masks, and had only one (paid) confidant in form of a psychotherapist who was willing to agree with her on everything.
Janet’s obsession with “wanting to be there completely” for her daughters’ final two years of school was placing a burden on her environment. She was at war with the headmaster, in particular regarding the laxer Covid protocols; teachers, concerning their methods and interactions; society at large for the cessation of vigilant pandemic measures she considered premature; her husband, whose despondence she could not attribute to her domination on all issues; and even her daughters’ search for privacy and independence, which she took personally in a highly emotional manner. Seemingly well-intentioned, her actions were socially disruptive. On a long-awaited family summer vacation, she prevented her daughters from mixing with peers out of fear that they would be drawn into illegal activities that the law would interpret differently with respect to them due to their ethnicity. Dinners were cut short when she felt others’ views were out of order, a frequent occurrence. Her daughters were showing signs of strain throughout the summer, one threatening self-harm and the other suffering from panic attacks. Both overcame their challenges with neurofeedback training.
Janet’s body began to give. A year after her daughters’ neurofeedback training, driven by the same ideals and obsessions, Janet began to experience cardiovascular issues. Heart dysrhythmia was diagnosed and treated with medication. She found it difficult to accept the advice of rest and detachment. Thoughts became intrusive, and even her therapist found the courage to voice their concerns about her trajectory to her. It was just before Christmas that she decided to reach out for neurofeedback training, whose success she’d witnessed in both her daughters.
We began with a brain map, which confirmed her relational thinking, mood and sleep disorders, various trauma markers, and sources of anxiety. Knowing, and fearing, that “this could change me”, we talked through the findings, which have an objective nature due to being based on physiology, or observed functional connectivity between brain areas, rather than being a subjective award of pathologies by an authority, for most of whom she harboured deep contempt. The fear, “could this change me”, had already been objectively overcome with her commitment to an initial brain map and session; subjectively, the prospect of achieving better sleep and reduced internal chatter had become sufficiently appealing.
As a former casting director, Janet retained her interest in art and theatre, and chose her favourite films to watch in session. Quickly engaged with the content, sessions felt non-invasive enough for her to tolerate. Neurofeedback sessions obviated the need for overt introflection, by contrast to talk therapy, and avoided triggering her with the result of reanimating her combative style. Her views were not questioned, and her brain trained to achieve a healthy sense of detachment in the first instance. This took a few sessions, during the course of which she noticed her sleep improving drastically. Being able to let go of her thoughts at night and settle into a deep state of relaxation was previously a feared scenario, yet this began to feel more natural and energising with every session. After five sessions, she noticed how her behaviour and reactions had began to change. No longer anticipating the worst in every situation, she felt a calm optimism and motivation that she could not recall having experienced for a long time. Relations with her supportive husband improved to everyone’s relief, and her daughters’ were positively surprised by her evolving lack of invasiveness. For the first time, it appeared that Janet was able to recall her own frustrations in her childhood at being micromanaged by her parents, and share this admission with her family. To everyone, it felt as if a weight was being lifted.
Encouraged by the positive feedback from her immediate environment, Janet continued with weekly neurofeedback sessions. At one point, she felt particularly emotional after a session, and found herself confiding in her brother on a long phone conversation that night. She felt lighter as a result, but was plagued with some remorse and guilt about how she had been acting. A supportive environment helped her achieve self-forgiveness and a more positive outlook. Reminded of her progress, she drew strength from the shape of her changed trajectory. It was as if people started to come closer to her, piercing an invisible wall she had built up around herself. Janet began to feel part of a social fabric that had an enabling quality and created a source of stability. Her moods and motivations became more stable, and she resumed interests in art that she had parked long ago. Within two months, Janet was talking to people from previous work-related circles who encouraged her to resume projects she had previously excelled in. Meetings followed, and melded into a social life. Physically, Janet felt better rested and ensconced in her body; hugs mattered, and her sensitivity was reciprocated. Embedded in a supportive environment, Janet began to flourish. Intrusive thoughts became ideas, and fears turned into surmountable challenges. She wished that she had begun training earlier, in parallel with her daughters, and was now living in the moment.
DSM-5 Definition of OCD
The DSM-5 defines Obsessive-Compulsive Disorder as follows:
Presence of obsessions, compulsions, or both:
Obsessions are defined by (1) and (2):
1. Recurrent and persistent thoughts, urges or images that are experienced, at some time during the disturbance, as intrusive, unwanted, and that in most individuals cause marked anxiety or distress.
2. The individual attempts to ignore or suppress such thoughts, urges, or images, or to neutralize them with some thought or action (i.e., by performing a compulsion).
Compulsions are defined by (1) and (2):
1. Repetitive behaviors (e.g., hand washing, ordering checking) or mental acts (e.g., praying, counting, repeating words silently) that the person feels driven to perform in response to an obsession, or according to the rules that must be applied rigidly.
2. The behaviors or mental acts are aimed at preventing or reducing distress or preventing some dreaded event or situation. However, these behaviors or mental acts either are not connected in a realistic way with what they are designed to neutralize or prevent or are clearly excessive.
The obsessions or compulsions are time consuming (e.g., take more than 1 hour per day) or cause clinically significant distress or impairment in social, occupational, or other important areas of functioning.
The disturbance is not better explained by the symptoms of another mental disorder (e.g., excessive worries, as in generalized anxiety disorder; preoccupation with appearance, as in body dysmorphic disorder; difficulty discarding or parting with possession, as in hoarding disorder; hair pulling, as in trichotillomania [hair-pulling disorder]; skin picking, as in excoriation [skin-picking] disorder); stereotypies, as in stereotypic movement disorder; ritualized eating behavior, as in eating disorders; preoccupation with substances or gambling, as in substance-related and addictive disorders; sexual urges or fantasies, as in paraphilic disorders; impulses, as in disruptive, impulse-control, and conduct disorders; guilty ruminations, as in major depressive disorder; thought insertion or delusional preoccupations, as in schizophrenia spectrum and other psychotic disorders; or repetitive patterns of behavior, as in autism spectrum disorder).
Specify if:
With good or fair insight: The individual recognizes that obsessive-compulsive beliefs are definitely or probably not true or that they may or may not be true.
With poor insight: The individual thinks obsessive-compulsive disorder beliefs are probably true.
With absent insight/delusional beliefs: The individual is completely convinced that obsessive-compulsive disorder beliefs are true.
Specify if:
Tic related: The individual has a current or past history of a tic disorder.
Neurofeedback is a form of complementary therapy and should not be seen as a replacement for conventional medicine. qEEG brain map-based neurofeedback training takes a more holistic approach to brain functioning, rather than just focusing on medical symptoms. It is not intended as a form of diagnosis nor medical intervention nor medical advice per the disclaimer.
Brain Maps and Personalised Brain Training Explained
Personalised Brain Training with Neurofeedback
Neurofeedback lets us train dysrythmic brain areas. With sensors comfortably fitted to the brain areas we want to train, we detect brainwave patterns real-time while watching a movie. When these patterns are inefficient, the volume drops momentarily. This is the feedback we are giving our brain, short and instantaneously.
The brain area we are training recognises this – while our conscious mind is focussed on the movie – and adjusts its behaviour to restore the normal volume. With repetition, throughout a session, learning occurs.
Meanwhile our conscious mind is solely focussed on the movie; the training process is passive in this sense.
The drop in volume is subtle, so we continue to understand the flow of the movie. No current or electrical stimulation is fed to the brain; sensors simply read brainwaves and the feedback is purely audio-visual.

Neurofeedback trains our Pre-Conscious Mind
Rather than engaging the conscious mind, which slows us down, we are training preconscious processes.
This equips us with the ability to live in the moment and attain our potential (if we have to resort to conscious control, we are not living in the moment).
We take a holistic approach to healthy brain self-regulation, rather than categorisation or diagnosis.
Personalised Brain Training is an advanced qEEG brain map-based approach to neurofeedback training developed by the founders of the field. Taking Othmer Method / ILF training methods further, it employs Default Network Training protocols as developed by David Kaiser.
Neurofeedback is Evidence-based
Neurofeedback training is an evidence-based complementary therapy. Its efficacy was first demonstrated some 50 years ago, and with advances in technology, training protocols have become more efficient and the feedback method – watching movies – thoroughly enjoyable.
Neurofeedback is evidence-based. It’s first application was discovered in 1971 when it was used to resolve intractable epilepsy.
There are over 2,000 peer-reviewed research reports on PubMed demonstrating efficacy across a number of pathologies.
In the US, it is an accepted complementary treatment for many challenges.